

June 15, 2026 — five papers at a glance
Primary quantitative findings
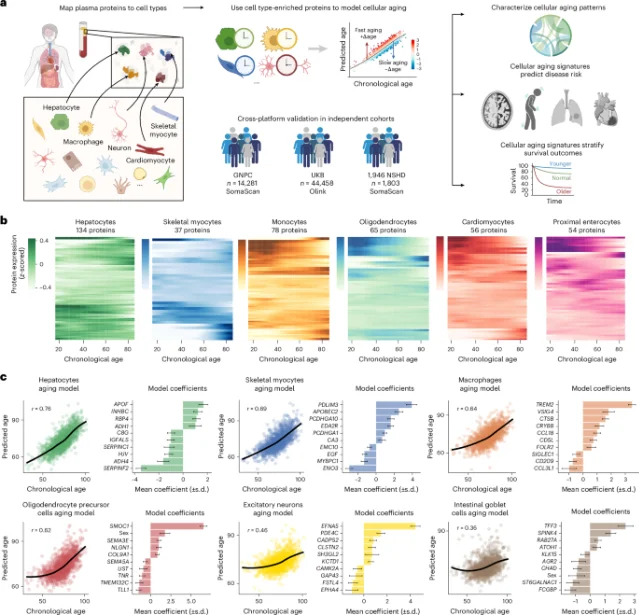
Plasma proteomics: extreme astrocyte aging hazard ratio for incident Alzheimer's disease (N=60,542)
0↑+5.2%95% CI 4.06–6.56; APOE4/4 with extreme astrocyte aging: 38.3% cumulative AD at 15 yr vs 0/23 with youthful astrocytes; ALS HR 12.74; lung cancer HR 15.33 in smokers
SODa-BIC: 30-day kidney MAKE composite — sodium bicarbonate arm (%)
0.0%↑+0.8%vs placebo 39.4%; adjusted difference +1.2 pp (95% CI −7.1 to 9.4); P=0.78 — null result; N=500, 55 ICUs, 7 countries
PPH: annual maternal deaths globally
0↑+0.0%27M women affected annually; vaginal prevalence 12.6%; cesarean 30.9%; ergometrine combinations no longer recommended (Cochrane NMA, 122 trials, 121,931 women)
CD3 bispecific Ab: treatment-related mortality across 104 trials, 10,353 patients (%)
0.0%↓−1.0%94/9,206 patients; I²=0.0%; causes: sepsis, pneumonia, neutropenic infection; any-grade CRS 43–46%; grade ≥3 TRAE 45–70%
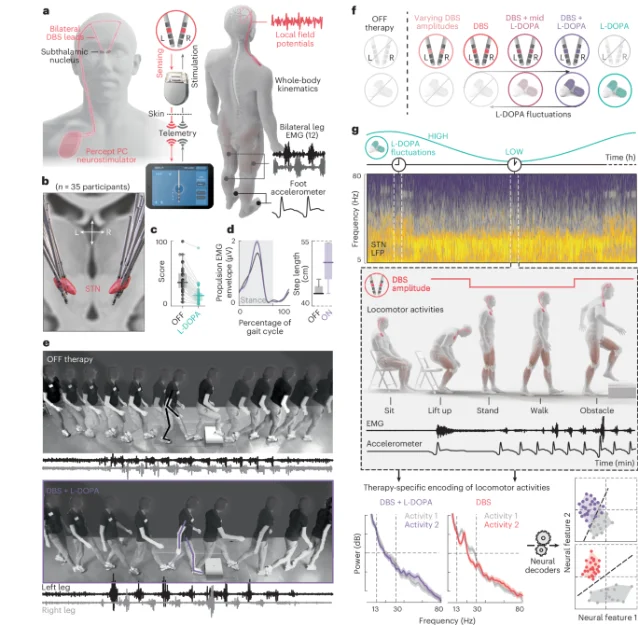
Adaptive DBS gait: fall reduction vs continuous DBS — odds ratio (Louie/Wang, N=3 crossover)
0+4.3%P=0.047 (95% CI 1.07–20.22); Scafa/Moraud: activity-dependent DBS improved gait in 4/4 refractory patients; +10.9% decoder F1-score gain
Add more perspectives or context around this Post.